

Abstract
Background
Altough the inhibitor of Bruton's tyrosyne kinase (BTK) ibrutinib has transformed the management of patients with CLL obtaining decreased tumor burden and improved progression free survival (PFS), it does not induce substantial apoptosis in vitro (Ponader, 2012). Dysregulation of the mitchondrial pathway of apoptosis is one of the hallmarks of CLL cell pathophysiology and thus targeting the anti-apoptotic protein bcl-2 with venetoclax is a promising new therapeutic strategy (Souers, 2013; Roberts, 2016). Moreover ibrutinib increases bcl-2 dependence (Deng, 2017) enhancing sensitivity to venetoclax in CLL. Therefore the basal level of apoptosis measured through bax/bcl-2 ratio before therapy may be crucial to test sensitivity to ibrutinib.
Aims
The primary aims of our research were: i) to verify the correlations of bax/bcl-2 ratio with other well-known biological and clinical prognosticators in patients treated with ibrutinib; ii) to evaluate the impact of bax/bcl-2 ratio on overall response rate (ORR), PFS and overall survival (OS); iii) to test bax/bcl-2 ratio as an independent prognostic factor.
Patients and Methods
Therefore, we evaluated the efficacy of ibrutinib, in a real-life contest, on 100 patients, median age 60 years (38-85), median number of previous regimens 2 (0-4; 14% previously untreated). Patients received 420 mg oral ibrutinib once daily until progression or occurrence of unacceptable side effects. Median follow up on ibrutinib was 16 months. ORR was 92% [complete response (CR): 27%, partial response (PR): 32%, PR with lymphocytosis (PR-L): 33%]. The estimate 1-year PFS and OS were 74% and 77%, respectively. Twenty-nine patients (29%) discontinued ibrutinib therapy due to progression (n=11) and serious adverse events (n=18). Five out of 6 patients with Richter's syndrome (RS) had baseline del(17p)/TP53 mutations (M). Interestingly, PFS was significantly better for patients in first/second lines (n=38) vs later lines of therapy (n=55; p=0.022). Bax/bcl-2 ratio was calculated by flow cytometry, dividing mean florescence intensity (MFI) of bax by MFI of bcl-2 on peripheral CLL cells before treatment with ibrutinib. The threshold of positivity was set at the median value higher than 1.5 (range 0.38-5.10).
Results
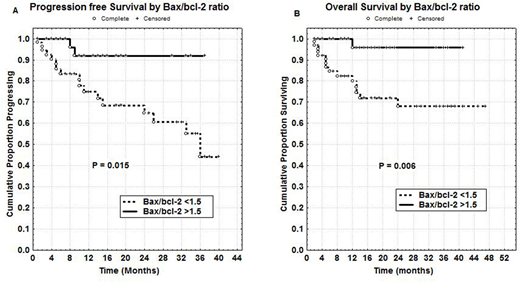
Sixty-four patients had bax/bcl-2 ratio <1.5 (64%). Bax/bcl-2 ratio <1.5 was strongly correlated with ZAP-70 >20% (40/64; p=0.005), but not with CD49d or CD38 >30%. There was only a slight significant correlation between bax/bcl-2 ratio <1.5 and NOTCH1 mutations (M) (25/32; p=0.030). On the other hand, no significant correlations were found between bax/bcl-2 ratio and del(17)p/TP53 M or IGHV status or cytogenetic subsets. With regard to clinical outcome, lack of response/progression and PR/PR-L were significantly correlated both with bax/bcl-2<1.5 (p=0.001) and NOTCH1 M (p=0.0005), but not with del(17)p/TP53 M. Noteworthy, 20/37 del(17)p/TP53 M patients were treated in first/second lines (p=0.001). Significant shorter PFS was observed in patients with bax/bcl-2 ratio <1.5 (65% vs 92% at 24 months, p=0.015, Figure A). Moreover, patients with lower bax/bl-2 ratio showed significant shorter OS (68% vs 96% at 24 months, p=0.006, Figure B). In multivariate analysis of PFS, only bax/bcl-2 ratio < 1.5 (p=0.030), analysed together with NOTCH1 M, TP53 M, number of therapeutic lines and age, was confirmed as an independent prognostic factor. With regard to multivariate analysis of OS, bax/bcl-2 ratio (p=0.016) and number of therapeutic lines (p=0.035) remained significant.
Conclusions
In our hands, bax/bcl-2 ratio was a powerful prognosticator for patients treated with ibrutinib, particularly useful to identify subsets of CLL patients with different levels of spontaneus apoptosis and consequent different clinical outcome under ibrutinib treatment. At the light of these our recent observations, bcl-2 antagonists, such as ABT-199, should be reasonably combined with BTK inhibitors, as it is already underway in clinical protocols, in order to overcome apoptosis resistance in patients treated with ibrutinib, particularly within the CLL subset characterized by lower bax/bcl-2 ratio e poor response to therapy with ibrutinib.
Del Principe:Gilead: Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal